Page: 1
/ 14
Total 139 questions
ARDMS AE Adult Echocardiography Examination AE-Adult-Echocardiography Exam Questions
Question 1
Which condition is commonly associated with cardiac tamponade?
Answer : D
Comprehensive and Detailed Explanation From Exact Extract:
Cardiac tamponade occurs when fluid accumulation in the pericardial space increases intrapericardial pressure, restricting ventricular filling and reducing cardiac output. A hallmark clinical feature is hypotension due to decreased stroke volume and cardiac output.
Jugular venous pressure is typically elevated (not decreased) because of impaired right heart filling. Tachycardia, not bradycardia, is usually present as a compensatory response. Blood pressure tends to be low or normal, not hypertensive.
This pathophysiology and clinical presentation are well documented in adult echocardiography literature and clinical cardiology textbooks, where tamponade is diagnosed with signs such as right atrial and ventricular diastolic collapse and associated clinical hypotension and elevated venous pressures16:Textbook of Clinical Echocardiography, 6ep.280-28512:ASE Pericardial Disease Guidelinesp.300-305.
Question 2
Which diagnosis is most likely confirmed by echocardiography in a 65-year-old female presenting with new onset chest pain associated with ST segment elevation on the electrocardiogram and angiographically normal coronary artenes?
Answer : D
Takotsubo cardiomyopathy, also known as stress-induced cardiomyopathy or 'broken heart syndrome,' predominantly affects postmenopausal women (usually older than 50 years) and often presents with acute chest pain and ST-segment elevation on the ECG mimicking acute myocardial infarction. However, coronary angiography reveals normal or non-obstructive coronary arteries.
Echocardiographically, Takotsubo cardiomyopathy is characterized by transient left ventricular systolic dysfunction with a typical pattern of apical ballooning and basal hyperkinesis. The wall motion abnormality extends beyond a single coronary artery territory, differentiating it from ischemic cardiomyopathy.
The diagnosis is supported by the clinical presentation, typical echocardiographic findings, and exclusion of obstructive coronary artery disease. The condition is usually reversible over days to weeks.
This is extensively described in the 'Textbook of Clinical Echocardiography, 6e' (Chapter 8: Coronary Artery Disease and Takotsubo Syndrome), which highlights the typical patient demographics, presentation, echocardiographic features, and prognosis .
Question 3
Which of the following does this Image represent?
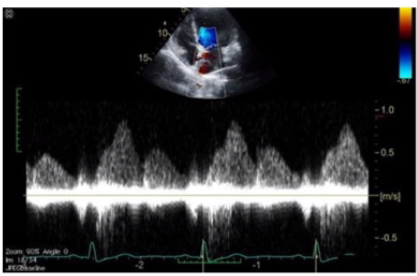
Answer : C
Comprehensive and Detailed Explanation From Exact Extract:
The image shows a pulsed-wave Doppler waveform with respiratory phasicity and distinct forward and reversed flow components characteristic of hepatic vein flow patterns. Hepatic vein Doppler typically displays a biphasic waveform with systolic (S) and diastolic (D) forward flow toward the heart and brief reversed flow during atrial contraction (A wave reversal), reflecting right atrial pressure changes.
Mitral and tricuspid inflow Doppler patterns show distinct E and A waves representing early and late diastolic ventricular filling but do not have the same flow reversal pattern. Pulmonary vein Doppler waveforms also differ, showing systolic and diastolic forward flows into the left atrium without the prominent reversed flow seen here.
The hepatic vein Doppler is commonly used in echocardiography to assess right atrial pressure and compliance, especially in conditions like constrictive pericarditis and right heart failure, where characteristic flow reversals and expiratory changes are observed.
This pattern and its clinical significance are detailed in adult echocardiography references, including the 'Textbook of Clinical Echocardiography' and ASE guidelines on Doppler imaging16:Hepatic Vein DopplerTextbook of Clinical Echocardiography, 6e12:ASE Doppler Guidelinesp.95-100.
Question 4
In patients with interrupted aortic arch, which structure allows Wood to flow into the descending aorta?
Answer : D
In interrupted aortic arch, the normal continuity between the ascending and descending aorta is disrupted. The patent ductus arteriosus (PDA) provides a vital conduit for blood to flow from the pulmonary artery to the descending aorta, maintaining systemic circulation distal to the interruption.
Persistent left superior vena cava and left carotid artery do not provide this flow. The foramen ovale is an atrial-level shunt and does not compensate for interrupted aortic arch.
This clinical anatomy is described in the 'Textbook of Clinical Echocardiography, 6e', Chapter on Congenital Aortic Arch Anomalies20:135-140Textbook of Clinical Echocardiography.
Question 5
Which flow component is indicated by the arrows on this image?
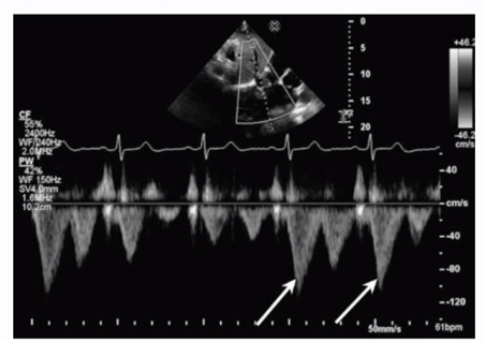
Answer : C
The Doppler waveform shows pulmonary vein flow with several components. The arrows point to small reversed flow spikes just after the atrial contraction wave, which corresponds to the atrial reversal (AR) flow component. Atrial reversal occurs as blood briefly flows backward into the pulmonary veins during atrial contraction.
Ventricular reversal is not typically seen in pulmonary veins. Diastolic flow reversal is abnormal and usually not part of normal pulmonary vein flow. Systolic forward flow is the major forward component during ventricular systole.
This interpretation is standard in ASE guidelines on diastolic function assessment and pulmonary vein Doppler evaluation12:ASE Diastolic Function Guidelinesp.85-9016:Textbook of Clinical Echocardiography, 6ep.130-135.
Question 6
Which of the following is the most likely cause for the findings demonstrated in this video?
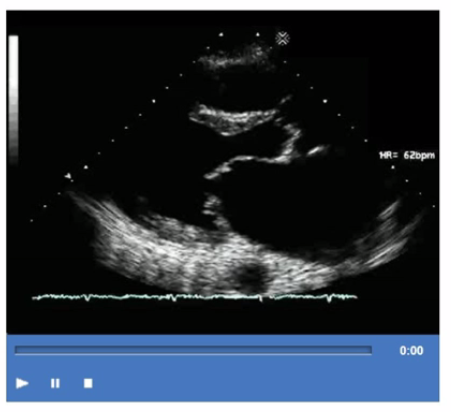
Answer : C
The video shows thickened, retracted, and possibly regurgitant valve leaflets with a characteristic appearance seen in drug-induced valvulopathy. Drugs such as ergot derivatives (e.g., methysergide) and appetite suppressants (e.g., fen-phen) can cause fibrotic thickening of valve leaflets mimicking carcinoid heart disease or rheumatic valve disease.
Infective endocarditis presents with vegetations and potentially valve destruction but typically not the diffuse thickening seen here. Rheumatic fever causes leaflet thickening but has a different chronic clinical course. Systemic lupus may cause valve thickening but often involves Libman-Sacks vegetations rather than diffuse fibrosis.
This is discussed in the 'Textbook of Clinical Echocardiography, 6e', Chapter on Valvular Heart Disease - Drug Induced and Secondary Causes20:400-405Textbook of Clinical Echocardiography.
Question 7
What is the normal dP/dt value of left ventricular systolic function?
Answer : D
Comprehensive and Detailed Explanation From Exact Extract:
The left ventricular dP/dt is a measure of the rate of rise in left ventricular pressure during isovolumic contraction, which reflects systolic function. It is derived from Doppler echocardiography by measuring the time interval between mitral regurgitant jet velocities of 1 m/s and 3 m/s. Using the simplified Bernoulli equation, the pressure gradient at each velocity is calculated, and the rate of pressure rise (dP/dt) is calculated by dividing the pressure difference by the time interval between these velocities.
A normal left ventricular dP/dt is generally considered to be greater than 1200 mmHg/s. Values lower than this indicate impaired systolic function, as the ventricle is slower to generate pressure during contraction.
For example, a measured time interval of 36 milliseconds (0.036 seconds) between the MR velocities of 1 and 3 m/s corresponds to a dP/dt of approximately 889 mmHg/s, which is mildly reduced, indicating some systolic dysfunction.
The exact extract from the 'Textbook of Clinical Echocardiography, 6e' states that normal dP/dt values are typically above 1000 mmHg/s, with >1200 mmHg/s considered a robust indicator of normal systolic function. This measure is useful but requires a measurable mitral regurgitation jet and consistent alignment of the ultrasound beam. Variability in measurement can occur based on technical factors, but the dP/dt remains a useful parameter to quantify systolic function noninvasively.